Saylor PT Huntersville
704-274-5795
Saylor Physical Therapy Huntersville
Pelvic Floor Therapy
Pelvic Floor Therapy at Saylor Physical Therapy Huntersville
What is the Pelvic Floor?
The pelvic floor is a combination of multiple muscles that begin at the pubic bone, bilateral to the ischial tuberosities or “sit bones”, and run all the way back to the tailbone. These muscles have ligamentous attachments creating a dome-shaped diaphragm across the boney pelvic outlet. The pelvic floor muscles have 5 main functions:
- Support of the pelvic organs- bladder, urethra, prostate (males), vagina and uterus (females), anus, and rectum, along with the general support of the intra-abdominal contents.
- Sphincteric support and contribution to continence of urine and feces
- Contribute to the sexual functions of arousal and orgasm
- Spine and pelvic stability
- Sump pump: pumping blood back from the heart
Elevation and support of the pelvic organs are associated with the pubococcygeus and the iliococcygeus. The pubococcygeus is the most medial component which separates, fashioning the levator hiatus with openings for the urethra, vagina (females), and anus. The bulbospongiosus and ischiocavernosus muscles are the primary contributors to the superficial portion of the pelvic floor. The more superficial musculature of the posterior pelvic floor constitutes the external anal sphincter. The transverse perineal muscles cross the mid-portion of the 1st layer of the pelvic floor and join with the bulbospongiosus muscles and external anal sphincter as the perineal body.
We can help you with your pelvic floor needs.



Pelvic Floor Therapy in Huntersville
Schedule an appointment and we look forward to providing you with quality, individual, one-on-one care for one full hour.
Typical PFM Dysfunctions
Our Therapists have experience working with a wide range of clientele for various PFM dysfunctions including:
-
Pain with Intercourse
-
Diastasis recti (separation in the abdomen)
-
Urinary/fecal leakage
-
Constipation
-
Bladder pain syndrome
-
Urinary/fecal urgency
-
Incomplete emptying of bladder/bowels
-
Pelvic pain associated with endometriosis
-
Antepartum/post-partum
-
Pelvic organ prolapse
-
Vulvodynia
-
Pelvic pain
-
Frequent urination/defecation
-
Scar restriction

Schedule an appointment for your pelvic floor needs
Pelvic Floor Issues
Diastasis recti:
Diastasis recti is an increased distance between the rectus abdominis muscles at the midline or linea alba caused by weakness in the anterior abdominal wall. Most experts agree that there is a weakness, thinning, and widening of the linea alba and weakness of the associated abdominal musculature.
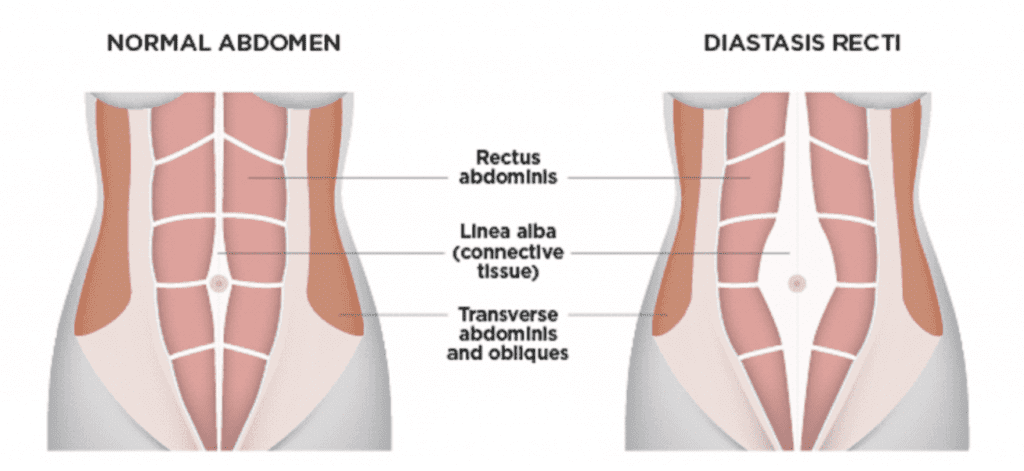
Some signs and symptoms caused by diastasis recti are common patient complaints including feeling of weakness or instability with any core work, noticing a bulge or coning in the abdomen, feeling of a separation in the abdomen. Diastasis recti has been shown to contribute to urinary stress incontinence and back pain.
Pelvic Organ Prolapse:
Pelvic organ prolapse is the descent of pelvic structures into the vagina due to ligament or muscular weakness. Pelvic organ prolapse (POP) is categorized according to the compartment of descent. Cystocele characterizes anterior wall descent/prolapse, rectocele refers to the posterior vaginal wall descent, and vaginal vault prolapse characterizes descent of the uterus, cervix, or apex of the vagina. They can occur either singly or in combination. Although the etiology of POP is multifactorial, there is a high correlation with pregnancy and vaginal delivery, which can lead to direct pelvic floor muscle and connective tissue injury.
Additionally, prior pelvic surgeries or conditions associated with sustained episodes of increased intrabdominal pressure such as heavy lifting, obesity, chronic cough, and constipation can increase the risk of developing POP. Most patients who present with prolapse are asymptomatic. However, symptoms become more bothersome as the bulge protrudes past the vaginal opening. Initial evaluation includes a detailed history and a systematic pelvic exam. An assessment of POP complications, including urinary incontinence, bladder outlet obstruction, and fecal incontinence, must be made.
Urinary Leakage:
Urinary incontinence is the involuntary leakage of urine. This medical condition is common in the elderly,but also affects younger adult males and females as well. Urinary incontinence can impact both patient health and quality of life. The prevalence may be underestimated as some patients do not inform health care providers of having issues with urinary incontinence for various reasons.
Several different types of urinary incontinence exist, including stress urinary incontinence, urge urinary incontinence, functional incontinence, mixed incontinence, and overflow incontinence. In most cases, urologic or gynecologic assessment is not necessary during the initial evaluation. The management of urinary incontinence depends on which type of incontinence is present and the severity of the symptoms.
1. Stress urinary incontinence is the involuntary leakage of urine that occurs with increases in intraabdominal pressure (e.g., with exertion, effort, sneezing, or coughing) due to urethral sphincter and/or pelvic floor weakness. Young women active in sports may experience this type of incontinence. In addition, pregnant women and women who have experienced childbirth may be prone to stress urinary incontinence.
2. Urge urinary incontinence is the involuntary leakage of urine that may be preceded or accompanied by a sense of urinary urgency (but can be asymptomatic as well) due to detrusor overactivity. The contractions may be caused by bladder irritation, poor habits, or loss of neurologic control. Signs of this may be rushing to the bathroom once an urge is felt, feeling urgency with triggers like turning the door knob or running cold water.
3. Mixed urinary incontinence is the involuntary leakage of urine caused by a combination of stress and urge urinary incontinence as described above.
4. Overflow urinary incontinence is the involuntary leakage of urine from an overdistended bladder due to impaired detrusor contractility and/or bladder outlet obstruction. Neurologic diseases such as spinal cord injuries, multiple sclerosis, and diabetes can impair detrusor function. Bladder outlet obstruction can be caused by external compression by abdominal or pelvic masses and pelvic organ prolapse, among other causes.
5. Functional urinary incontinence is the involuntary leakage of urine due to environmental or physical barriers to toileting. This type of incontinence is sometimes referred to as toileting difficulty.
Constipation:
Constipation is defined as infrequent passage of stools or difficulty with evacuation of stools. It is associated with various symptoms including hard stools, straining, sensation of anorectal blockage, incomplete evacuation, abdominal discomfort, and bloating. The prevalence of constipation has a higher female to male ratio and a higher prevalence in the elderly especially over 65 years.
Causes of constipation can be divided into primary (slow transit or outlet obstruction) or secondary causes. Secondary causes can include simple dehydration or inadequate fluid intake, metabolic disturbances, medications, neurological disorders, myopathic disorders and structural abnormalities.
Pelvic Floor Therapy in Huntersville
Contact us for more information or to schedule your appointment today
Services at Saylor Physical Therapy Huntersville
Neck & Back
Pain
Shoulder, Elbow
& Hand Pain
Hip & Knee
Pain
Foot & Ankle
Pain
Sports Therapy &
Injury Therapy
Pelvic Floor
Therapy
contact saylor pt Huntersville
Get In Touch
new to Saylor PT Huntersville?
new patients
Address
Saylor PT Huntersville
13620 Reese Blvd East
Suite 130
Huntersville, NC 28078
Phone
P 704-274-5795
F 704-274-5750
Hours
Mon 7 am–7 pm
Tues 7 am–7 pm
Wed 7 am–7pm
Thu 7 am–7 pm
Fri 7 am–7 pm
Sat Closed
Sun Closed